Why ADHD Treatment Fails in Some Adults
- joeudesign
- May 20
- 8 min read

You followed the prescription. You showed up to appointments. You did what you were supposed to do. And yet, something still feels off. Understanding why ADHD treatment fails in some adults is not about finding blame. It’s about recognizing that ADHD in adults is far more complex than a simple chemical imbalance that one pill can fix. This article breaks down the real reasons treatment falls short and what you can actually do about it.
Table of Contents
Key Takeaways
Point | Details |
Pharmacoresistance is real | About 30% of adults with ADHD see minimal benefit from medication despite correct dosing. |
Genetics affect drug response | CYP2D6 gene variations change how your body processes ADHD medications, making standard doses ineffective for some. |
Comorbidities complicate outcomes | Anxiety, depression, and sleep disorders can mask or amplify ADHD symptoms, undermining treatment. |
Medication alone is rarely enough | Symptom severity, not medication status, drives cognitive and functional deficits in adults. |
Multimodal care works better | Combining behavioral therapy with medication lowers the required drug dose while improving daily functioning. |
Why ADHD treatment fails in some adults
The most common assumption is that if a medication is prescribed correctly and taken consistently, it should work. For many adults, that assumption turns out to be wrong, and the reasons go deeper than most people expect.
Pharmacoresistance is one of the least-discussed causes. About 30% of individuals with ADHD experience suboptimal outcomes due to pharmacoresistance, meaning their brain simply does not respond adequately to standard medications despite correct dosing and adherence. This is not a willpower problem. It is a biological one.
Genetics play a significant role here. CYP2D6 polymorphisms are genetic variations that affect how your liver metabolizes stimulant medications. If you are a “rapid metabolizer,” the drug clears your system too quickly to be effective. If you are a “poor metabolizer,” even standard doses can accumulate to problematic levels. Neither scenario shows up on a standard prescription.
Comorbid conditions add another layer of complexity. Adults with ADHD frequently live with anxiety, depression, and sleep disorders that either mask ADHD symptoms or amplify them in ways that make treatment harder to calibrate. Treating ADHD without addressing these conditions is like trying to fix a leak while the water keeps running.
Non-adherence is also a hidden factor. Treatment coverage drops to as low as 8% to 30% after two years across different countries, meaning most adults quietly drift away from their regimens without ever telling their provider. Missed doses and inconsistent schedules create gaps that look like medication failure but are actually adherence failure.
Pharmacoresistance affects roughly 1 in 3 adults with ADHD
Genetic metabolism differences change how drugs work in your body
Comorbid anxiety and depression distort symptom presentation
Inconsistent medication use creates the illusion of treatment failure
Dosing variability between medication types adds unpredictability
Pro Tip: If your medication feels like it stopped working, ask your prescriber about pharmacogenomic testing. A simple cheek swab can reveal whether your genetics are affecting how you process the drug.
How symptom severity shapes your outcomes
Here is something that surprises many people: being on medication does not automatically mean your cognitive deficits will improve. A major 2026 study found that symptom severity drives deficits in daily functioning, not whether someone is medicated or not. Medicated and unmedicated adults with similar symptom severity showed comparable levels of impairment. That is a significant finding that reshapes how we should think about ADHD treatment challenges adults face.

What this means practically is that adults with more severe ADHD symptoms experience greater cognitive and motor impairments regardless of their medication status. Executive function struggles, including planning, time management, and impulse control, do not automatically resolve once a stimulant kicks in. Visuospatial skills and motor coordination, which affect everything from driving to organizing a workspace, are often overlooked entirely in standard treatment plans.
The problem is that most ADHD evaluations focus on symptom checklists rather than neurocognitive profiles. Two adults can score similarly on a symptom scale but have completely different patterns of functional impairment. One person might struggle most with working memory. Another might have significant problems with emotional regulation. A one-size prescription approach fails both of them.
Personalized treatment plans built around individual neurocognitive profiles are what the research now points toward. This means assessing not just symptom frequency but the specific cognitive domains where someone struggles most, then targeting those areas directly through both medication and non-medication strategies.
Executive function deficits (planning, prioritizing, initiating tasks)
Working memory impairments affecting follow-through
Emotional dysregulation that medication rarely fully addresses
Motor coordination issues that impact daily tasks
Visuospatial processing challenges often missed in standard evaluations
The takeaway is not that medication is useless. It is that medication treats a portion of the problem, and the rest requires targeted, personalized support.
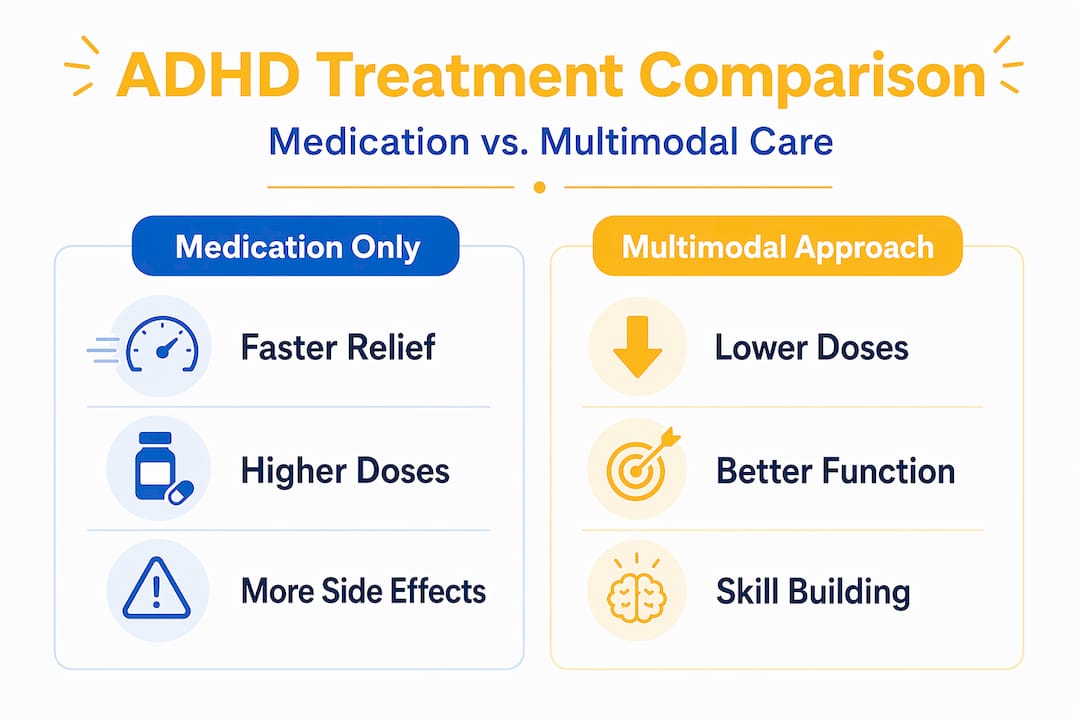
Medication-only vs. multimodal treatment
This is where the data gets genuinely interesting. Stimulant medications do work, and they work well in the short term. Acute efficacy is strong, with standardized mean differences of 0.81 to 1.10 in controlled trials. But the picture changes over time.
Approach | Strengths | Limitations |
Stimulants only | Fast symptom relief, well-studied | No significant long-term reduction by early adulthood; cardiovascular and growth risks |
Non-stimulants only | Fewer abuse concerns, useful for comorbidities | Slower onset, often less potent for core symptoms |
Behavioral therapy only | Builds lasting skills, no side effects | Slower results, requires consistent effort and access |
Combined treatment | Lower drug doses needed, better functional outcomes | Requires more coordination between providers |
Extended stimulant use carries real physiological costs, including an average height suppression of 2.55 cm and a cardiovascular risk increase with an incidence rate ratio of 1.41 within six months of use. These are not reasons to panic, but they are reasons to reconsider whether medication alone is the right long-term strategy.
The combined approach changes the math significantly. Combined treatment reduces the average stimulant daily dose from 37.7 mg to 31.2 mg while maintaining symptom control. Behavioral therapies improve organizational skills with a standardized mean difference of 0.85. You get better outcomes with less medication exposure.
Non-stimulant options like atomoxetine and guanfacine are worth knowing about too. They work differently, targeting norepinephrine pathways rather than dopamine, and they carry different side effect profiles. For adults with comorbid anxiety or a history of substance use, they can be a better fit even if the symptom relief feels less immediate.
Pro Tip: When evaluating your treatment plan, ask your provider specifically about organizational skills training and behavioral coaching. These are not just “therapy add-ons.” They address the functional gaps that medication alone does not fill.
Practical strategies when treatment is not working
When you feel like your treatment has hit a wall, the worst thing you can do is quietly give up. Medication failure is not just about symptom reduction. It is about losing your grip on daily functioning, and that requires a thorough clinical reassessment, not just a dose adjustment.
Here is a practical framework for moving forward:
Request a comprehensive reassessment. Ask your provider to evaluate not just symptom frequency but functional impairment across work, relationships, and daily tasks. Bring specific examples of where you are struggling.
Explore medication adjustments. This might mean switching between stimulant classes, trying a non-stimulant, or investigating whether genetic testing could explain your response pattern.
Add behavioral support. Cognitive behavioral therapy adapted for ADHD, executive function coaching, and skills-based training address the gaps medication leaves open.
Prioritize sleep. Sleep deprivation mimics and worsens ADHD symptoms. Poor sleep hygiene can make even effective medication look like it is failing.
Get consistent exercise. Aerobic exercise increases dopamine and norepinephrine naturally. Research consistently supports it as a meaningful adjunct to medication, not a replacement but a genuine booster.
Address comorbidities directly. If anxiety or depression is present, treating those conditions separately often improves ADHD treatment response significantly.
Non-specific factors like motivation levels and comorbid anxiety meaningfully influence ADHD treatment outcomes beyond what medication alone can address. This is why a holistic view of your mental health matters so much when evaluating common ADHD treatment obstacles.
Pro Tip: Keep a simple weekly log tracking your mood, sleep hours, medication timing, and focus quality. Patterns in that data will give your provider far more useful information than a 15-minute appointment alone.
My take on why personalized care changes everything
I have seen a consistent pattern across adults who struggle with ADHD treatment. The ones who feel most frustrated are almost always the ones who were handed a prescription and told to come back in three months. That model works for some people. For many, it does not.
What I have learned is that the adults who improve most are the ones whose care accounts for who they actually are, not who the average clinical trial participant was. Pharmacoresistance, genetic metabolism differences, and comorbid conditions that complicate medication response are not edge cases. They are common realities that standard protocols often miss.
The 2026 research on symptom severity genuinely shifted how I think about this. Medication is a tool, not a solution. When you treat it like a solution, you set yourself up for disappointment. When you treat it like one component of a broader plan, outcomes improve.
My advice is to advocate loudly for a treatment plan that includes behavioral support, lifestyle factors, and regular reassessment. You are not asking for too much. You are asking for what the evidence actually supports. And if your current provider is not open to that conversation, finding one who is may be the most important step you take.
— Martin
Ready to get a treatment plan that actually fits you?
If you have been cycling through medications without lasting results, or if you feel like your provider has never quite understood the full picture of what you are dealing with, 2ndarc was built for exactly that situation.
2nd Arc Psychiatric Associates offers personalized psychiatric care that goes beyond a prescription pad. The clinical team creates custom treatment plans that integrate medication management, behavioral support, and lifestyle strategies tailored to your specific neurocognitive profile. With both in-person and telehealth options across New York and appointments often available within 24 hours, getting a real assessment does not have to be a months-long wait. Most major insurance plans are accepted. If your ADHD treatment has not been working, a fresh evaluation from a team that takes the full picture seriously could be the turning point.
FAQ
Why does ADHD medication stop working over time?
Tolerance, changes in metabolism, and evolving comorbid conditions can all reduce medication effectiveness over time. Treatment coverage drops significantly after two years, often because adults stop taking medication consistently rather than because the drug has truly stopped working.
Can genetics explain why my ADHD medication isn’t effective?
Yes. CYP2D6 genetic polymorphisms affect how your body metabolizes stimulant medications, meaning standard doses may clear your system too quickly or accumulate to uncomfortable levels depending on your genetic profile.
Is behavioral therapy necessary if I’m already on medication?
Research strongly suggests yes. Combined treatment improves functional outcomes and allows for lower medication doses, addressing the organizational and executive function deficits that stimulants alone do not reliably fix.
How do comorbidities affect ADHD treatment outcomes?
Conditions like anxiety, depression, and sleep disorders can mask ADHD symptoms or make them worse, creating a moving target for treatment. Addressing these conditions alongside ADHD, rather than treating them separately, tends to produce better results for both.
What should I do if my current ADHD treatment isn’t working?
Request a comprehensive reassessment that includes functional impairment, not just symptom frequency. Explore medication adjustments, ask about pharmacogenomic testing, and discuss adding behavioral support or lifestyle interventions to your plan.
Recommended



Comments